
Current cancer therapies often fail to prevent later relapses. Moreover, they fail to treat metastatic disease. We believe that by targeting the sources of those metastases we can prevent metastasis formation. What are these source cells? Our investigation provides evidence that the source of metastasis are cancer cells that have left the primary site (i.e. mammary gland tissue) and arrived at secondary organs such as bones. We have also shown that these disseminated cancer cells (also called DCCs) remain in a non-proliferative state for extended periods of time. We name this non-proliferative state as dormancy. However, upon unknown signals these DCCs start to proliferate and become metastasis. Therefore, if we understand how these cells reactivate we might have a chance to stop these DCCs from becoming a life-threatening metastasis.
To add more complexity to the biology of DCCs, our previous publications, using a mouse model of HER2 oncogene overexpression, showed that DCCs population is composed, at least, of two types of cells. Those coming from early cancer cell lesions (early DCCs) and those coming from invasive primary tumors (late DCCs). This indicates that before a tumor is detected patients may have already early DCCs at secondary organs (i.e. bone marrow). Therefore, we need to understand how these two populations of DCCs contribute to metastasis formation.
The laboratory focuses on determine the mechanisms that control tumor dormancy of residual disease. Specifically, we aim to 1- understand how residual tumor cells enter dormancy, how they reactivate from dormancy and how they survive; 2- to identify the origins of DCCs and determine the type of DCC that contributes to lethal metastases so we can propose strategies to prevent metastasis formation. These findings will contribute to the paradigm shift on the origins and biology of cancer metastasis and this would impact significantly how we target the precursors of metastasis to prevent this lethal stage of the disease.
DISSEMINATION DURING EARLY STAGE OF BREAST CANCER PROGRESSION
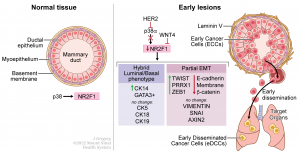
The current challenge for the management of treatment of early-stage breast cancer patients (for instance, patients carrying ductal carcinoma in situ, DCIS which are considered non-invasive lesions) is that even though local invasive recurrences are reduced after surgery or surgery with radiation, the risk of dying from breast cancer remains the same. This suggests that before detection and removal of the invasive tumor mass some pre-malignant cells disseminated and lodged at other sites waiting for later reactivation. The identification of an ‘early dissemination signature’ in the breast tissue that could identify patients with risk of developing later relapses, and are therefore candidates for systemic therapy, is crucial to reduce mortality in these patients. This study (DOI: 10.1158/0008-5472.CAN-21-4145) reveals the mechanisms by which pre-malignant cancer cells acquire mobile and invasive features that allow dissemination and colonization in other organs.